
Lymphedema Guide
Lymphedema: Causes, Pathophysiology, Diagnosis and Therapy
Lymphedema is not just simple swelling. It is a chronic and progressive disease of the lymphatic system that requires early diagnosis, consistent therapy and lifelong management. In this article, we explain what causes lymphedema, how it progresses, how it is diagnosed and which therapies can help slow or stabilise the condition.
What lymphedema is
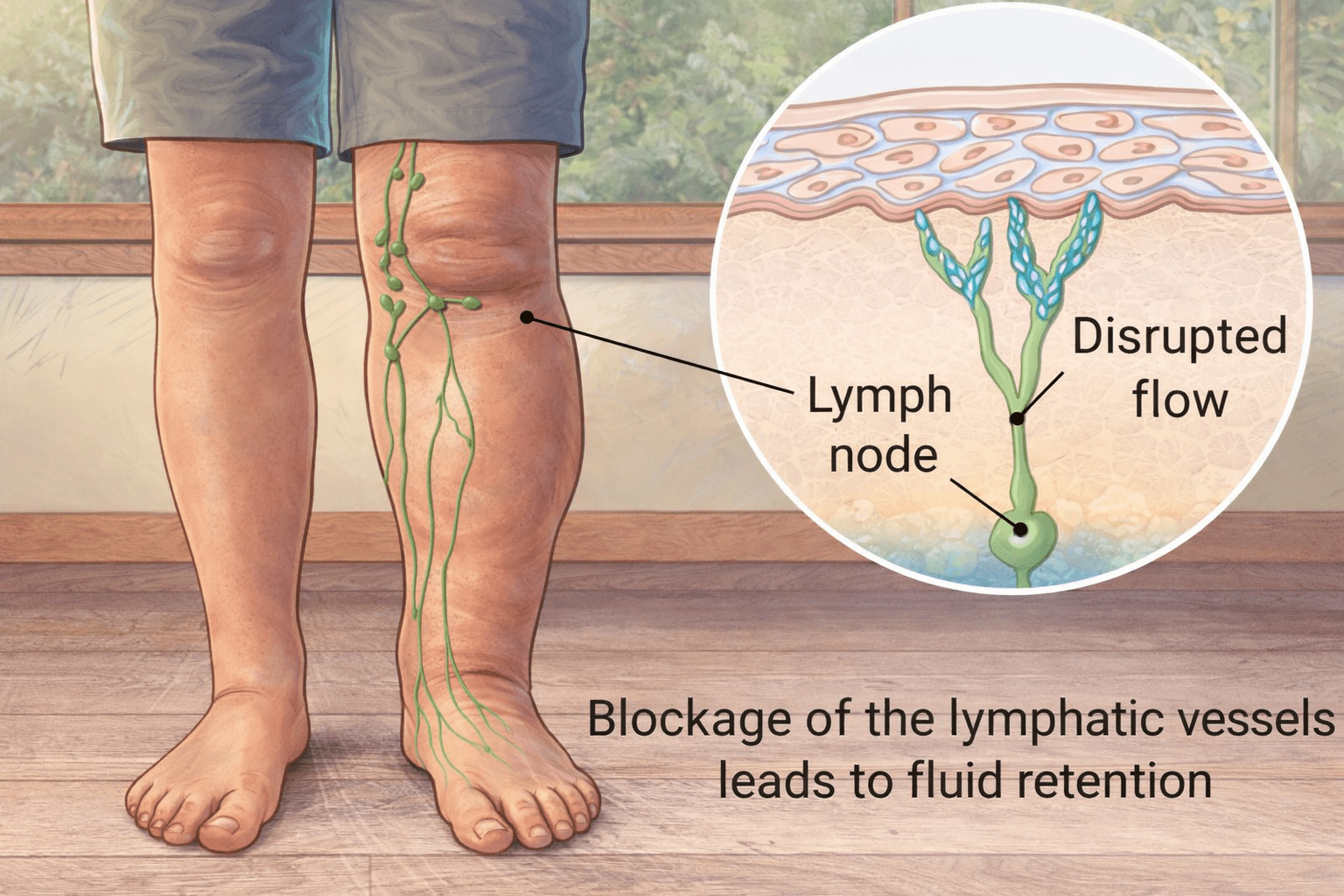
Lymphedema is a chronic and progressive disease of the lymphatic system. It results from an insufficiency of lymph transport capacity and is characterised by the accumulation of protein-rich interstitial fluid.
This accumulation leads to persistent tissue swelling, chronic inflammation, fibrosis and an increased risk of infections. Unlike transient or venous edema, lymphedema is not self-limiting and does not resolve spontaneously. Once established, it requires lifelong management.
Clinically, lymphedema most frequently affects the extremities, particularly the arms and legs. It may also involve the trunk, head, neck or genital region.
Over time, untreated or insufficiently treated lymphedema can lead to progressive tissue remodelling, skin changes and functional impairment, significantly reducing quality of life.
Etiology and classification
Lymphedema is classified as either primary or secondary, depending on its underlying cause.
Primary lymphedema
Primary lymphedema is caused by congenital malformations of the lymphatic system. These may include hypoplasia, aplasia or structural abnormalities of lymph vessels and lymph nodes.
Primary forms typically present at birth, during puberty or in early adulthood and predominantly affect women. The lower extremities are most commonly involved, often unilaterally. The swelling usually begins distally and progresses proximally over time.
Secondary lymphedema
Secondary lymphedema develops as a result of acquired damage to an initially intact lymphatic system.
In industrialised countries, the most common causes are oncological interventions, particularly surgical removal of lymph nodes and radiotherapy.
Additional causes include trauma, burns, recurrent infections, inflammatory processes, malignant tumours compressing lymphatic pathways and, in some regions, parasitic infections such as filariasis.
When no clear cause can be identified, the condition is described as idiopathic lymphedema.
Physiology of the lymphatic system
Under physiological conditions, blood circulation continuously delivers oxygen and nutrients to tissues while removing metabolic waste products.
At the level of the capillaries, fluid is filtered into the interstitial space. Approximately ninety percent of this fluid is reabsorbed directly into the venous system.
The remaining ten percent, amounting to six to ten litres per day, remains in the interstitial space and must be removed by the lymphatic system.
This residual fluid, known as lymph, contains plasma proteins, lipids, immune cells, cellular debris, microorganisms and foreign particles.
The lymphatic system begins as a network of open-ended lymph capillaries embedded in the connective tissue. Through pressure gradients, tissue movement and intrinsic vessel contractility, lymph is absorbed and transported through pre-collectors, collectors and lymph nodes before being returned to the venous circulation.
Beyond fluid balance, the lymphatic system is a central component of immune defence.
Lymph nodes function as filtration and immune activation sites, enabling the recognition and elimination of pathogens and foreign substances.
Pathophysiology of lymphedema
Lymphedema develops when the transport capacity of the lymphatic system is reduced below the required load. This may occur due to structural damage, functional impairment or both.
As lymph transport becomes insufficient, protein-rich fluid accumulates in the interstitial space.
The presence of proteins in the tissue initiates a chronic inflammatory response. Fibroblasts are activated, leading to progressive fibrosis, while adipose tissue deposition increases over time.
These changes explain why lymphedema gradually becomes firmer, less compressible and increasingly resistant to treatment if not addressed early.
Diuretics are ineffective because they do not remove proteins from the interstitial space and may even worsen tissue changes.
Clinical staging
Lymphedema progresses through several clinically defined stages.
Latent stage
In the latent stage, lymphatic damage is already present, but no visible swelling can be detected. Functional diagnostic methods may reveal impaired lymph transport.
Reversible stage
In the reversible stage, soft swelling is present and pitting can be induced by pressure. Elevation of the affected limb leads to a temporary reduction in swelling.
Spontaneously irreversible stage
As the disease progresses, tissue fibrosis increases, pitting becomes difficult or impossible, and swelling no longer resolves with elevation.
Elephantiasis
In the most advanced stage, known as elephantiasis, massive swelling, pronounced skin changes and severe functional limitations occur.
Diagnostic principles
The diagnosis of lymphedema is primarily clinical and is based on a detailed medical history and physical examination.
Imaging techniques such as lymphoscintigraphy or indocyanine green lymphography may be used in unclear cases or for treatment planning.
Ultrasound and magnetic resonance imaging are helpful in excluding differential diagnoses such as venous disease or tumours.
Complex Physical Decongestive Therapy
The internationally accepted gold standard for the treatment of lymphedema is Complex Physical Decongestive Therapy, also known as CPT, Complex Physical Therapy or KPE.
CPT consists of four interdependent components:
- Manual lymph drainage
- Compression therapy
- Exercise therapy
- Meticulous skin care
These elements must be applied in a coordinated and consistent manner to achieve effective and sustainable results.
Manual lymph drainage
Manual lymph drainage is a specialised therapeutic technique designed to stimulate lymph transport.
A fundamental principle of effective MLD is that treatment must always begin centrally, at the level of the neck. This region contains the venous angles where lymph enters the bloodstream.
Clearing central lymphatic pathways first creates a suction effect that allows lymph from peripheral regions to drain effectively.
If central clearance is neglected, peripheral drainage techniques are largely ineffective. Incorrectly performed MLD provides no therapeutic benefit and represents a misuse of time and resources.
To maintain its effect, MLD must always be combined with compression therapy.
Compression therapy
Compression therapy is the most decisive and effective component of lymphedema treatment.
By increasing tissue pressure, compression reduces capillary filtration, enhances lymph uptake, redistributes interstitial fluid and activates the muscle and joint pump during movement.
It also improves microcirculation, reduces oxidative stress and contributes to the softening of fibrotic tissue.
Because compression garments are worn for many hours each day, they provide thousands of hours of therapeutic effect per year.
Treatment phases
CPT is divided into two distinct phases: the decongestion phase and the maintenance phase.
During the decongestion phase, the primary goal is maximal volume reduction. This phase involves frequent manual lymph drainage combined with compression bandaging or adaptive compression systems that can be adjusted as limb volume changes.
Once no further volume reduction can be achieved, treatment enters the maintenance phase. The goal at this stage is long-term stabilisation.
Custom-made flat-knit compression garments are required to maintain the achieved results. These garments provide low resting pressure and high working pressure, allowing effective lymph flow during movement without compromising arterial circulation.
They must only be prescribed after sufficient decongestion has been achieved.
Exercise and respiratory therapy
Exercise performed while wearing compression is an essential component of lymphedema management.
Muscle contraction increases tissue pressure and promotes the transport of lymph and venous blood toward the heart.
Respiratory therapy further enhances lymph flow, particularly through the thoracic duct, the largest lymphatic vessel in the body.
Diaphragmatic breathing acts as a powerful physiological pump that supports central lymphatic drainage.
Intermittent pneumatic compression
Intermittent pneumatic compression may be used as an adjunctive therapy to support decongestion.
Suitable devices apply sequential, distal-to-proximal pressure through multiple overlapping chambers.
When used correctly, IPC can enhance lymph transport and reduce the frequency of manual lymph drainage sessions. Improper devices or incorrect use may worsen edema and must be avoided.
Infections in lymphedema and erysipelas
In patients with lymphedema, susceptibility to infections is markedly increased, with erysipelas being the most frequent and clinically significant complication.
The impaired lymphatic system reduces local immune surveillance, while protein-rich interstitial fluid provides an optimal environment for bacterial growth.
At the same time, chronic swelling compromises the skin barrier, leading to dryness, fissures and microlesions that facilitate bacterial entry.
Erysipelas often presents with acute onset, systemic symptoms such as fever and a painful, sharply demarcated erythema of the affected limb.
Even minor skin injuries, including small cuts, insect bites, interdigital fissures or fungal infections, can trigger an episode.
Each occurrence of erysipelas further damages lymphatic vessels, increases scarring and permanently reduces lymph transport capacity.
Recurrent infections therefore play a central role in disease progression, accelerating fibrosis, increasing limb volume and significantly worsening long-term outcomes.
Skin care and infection prevention
Effective infection prevention is a core component of lymphedema management and must be considered equally important as edema reduction itself.
In lymphedema, the immune defence of the affected tissue is compromised, and the skin barrier is often impaired.
Consistent skin care is therefore essential to reduce infection risk. Gentle cleansing, thorough drying, lipid-replenishing products and avoidance of irritants help maintain skin integrity and limit bacterial entry points.
Selenium and immune support
Selenium is an essential trace element required for immune function and antioxidant defence. In patients with lymphedema, selenium deficiency may further impair local immune responses and increase susceptibility to infections.
Scientific studies have demonstrated that sodium selenite supplementation, when combined with CPT, can accelerate edema reduction, reduce tissue fibrosis and significantly lower the recurrence rate of erysipelas.
In clinical studies, patients receiving sodium selenite showed fewer infectious episodes compared to those treated with CPT alone, alongside measurable improvements in skin condition and quality of life.
Selenium supplementation should be considered in patients with recurrent erysipelas or confirmed selenium deficiency. Due to its narrow therapeutic range, supplementation must be medically supervised.
When appropriately used, selenium represents a valuable adjunct in the comprehensive management of lymphedema.
Patient education and long-term management
Lymphedema is not curable, but it is controllable. Long-term success depends heavily on patient education and adherence to therapy.
Understanding the underlying mechanisms of the disease, the purpose of each therapeutic component and the consequences of inadequate treatment enables patients to actively participate in their care.
Educated patients show better adherence, fewer complications and improved quality of life.
Key takeaways
- Lymphedema is a chronic and progressive disease of the lymphatic system.
- It can be primary or secondary, depending on the underlying cause.
- Early diagnosis and consistent therapy can slow or stabilise progression.
- Complex Physical Decongestive Therapy is the accepted gold standard.
- Compression therapy is one of the most important long-term treatment components.
- Skin care and infection prevention are essential parts of management.
- Patient education is central to long-term success.
Conclusion
Lymphedema is a complex systemic disease rather than a simple swelling disorder.
Effective management requires a deep understanding of lymphatic physiology, structured lifelong therapy, proactive infection prevention and active patient involvement.
When treated correctly and consistently, disease progression can be slowed, complications, particularly infections, can be minimised, and long-term quality of life can be preserved.
Sources and references
The content of this article is based on and scientifically informed by peer-reviewed clinical articles published in the German specialist journal Lymphe & Gesundheit, a professional publication dedicated to lymphology, lymphedema and related disorders.
Primary sources
-
Lymphe & Gesundheit, Issue 01/2010
Das Lymphödem und seine Behandlung – Teil 1
Focus: definition, physiology of the lymphatic system, pathophysiology, staging and principles of complex physical decongestive therapy. -
Lymphe & Gesundheit, Issue 03/2025
Lymphödeme – Ursachen, Diagnose, Therapie – Teil 2
Focus: advanced therapy concepts, infections in lymphedema, erysipelas, selenium supplementation, immune aspects and long-term management. -
Selen in der Behandlung von Lymphödemen
Published in Lymphe & Gesundheit.
Official source and download page: Lymphe & Gesundheit downloads
Try Ynone for free
Join the app waiting list
Be among the first to try Ynone and help shape a digital support tool for lymphedema self-management.
Join the waiting list